Article Text

Abstract
Objective The aim of the meta-analysis was to determine the association of obesity and heart failure (HF) and the cardiac impact of intentional weight loss following bariatric surgery on cardiac structure and myocardial function in obese subjects.
Methods MEDLINE, Embase and Web of Science were searched up to 3 April 2018. Studies reporting association and prognostic impact of obesity in HF and the impact of intentional weight loss following bariatric surgery on cardiac structure and myocardial function in obesity were included in the meta-analysis.
Results 4959 citations were reviewed. After exclusions, 29 studies were analysed. A ‘J curve’ relationship was observed between body mass index (BMI) and risk of HF with maximum risk in the morbidly obese (1.73 (95% CI 1.30 to 2.31), p<0.001, n=11). Although ‘obesity paradox’ was observed for all-cause mortality, the overweight group was associated with lower cardiovascular (CV) mortality (OR=0.86 (95% CI 0.79 to 0.94), n=11) with no significant differences across other BMI groups. Intentional weight loss induced by bariatric surgery in obese patients (n=9) without established HF, atrial fibrillation or known coronary artery disease, was associated with a reduction in left ventricular mass index (p<0.0001), improvement in left ventricular diastolic function (p≤0.0001) and a reduction in left atrial size (p=0.02).
Conclusions Despite the increased risk of HF with obesity, an ‘obesity paradox’ is observed for all-cause mortality. However, the nadir for CV mortality is observed in the overweight group. Importantly, intentional weight loss was associated with improvement in indices of cardiac structure and myocardial function in obese patients.
Trial registration number APP 74412.
- obesity
- heart failure
- obesity paradox
- weight loss
Statistics from Altmetric.com
Introduction
Obesity is a modern-day epidemic affecting more than one-third of the population worldwide.1 Similarly, heart failure (HF) is a major public health problem with an estimated lifetime risk of one in five. Obesity is considered to contribute to the increasing incidence of all subgroups of HF.2 However, there have been variable reports on the impact of obesity on HF prognosis.3 Though wasting in terminal HF patients has been associated with poor prognosis, a recent bariatric surgery study has shown that intentional weight loss in obese patients is associated with reduced risk of incident HF.4 5 The present ACCF/AHA society guidelines appreciate that obesity is a risk factor for HF but do not have firm recommendations on weight management in HF.6
Therefore, a potential beneficial impact of intentional weight loss in obese patients continues to be a issue of conjecture but worth investigating given the benefit observed in other patient populations such as atrial fibrillation (AF).7 8 The purpose of this systematic review and meta-analysis is to evaluate the relationship between obesity and the incidence of HF and its impact on prognosis in HF in the general population and to explore the impact of intentional weight loss in obese individuals on indices of cardiac structure and function by bariatric surgery.
Methods
This systematic review complies with the Meta-analysis of Observational Studies in the Epidemiology group and Preferred Reporting Items for Systematic Review and Meta-Analysis statements. The meta-analysis was registered with PROSPERO International register for systematic reviews (APP 74412).
Search strategy
The English scientific literature was searched using PubMed, Embase and Web of Science between the period 1 January 1950 to 3 April 2018 with the assistance of an experienced librarian. The following keywords were used ‘Obesity’, ‘abdominal obesity’, ‘Diabetic Obesity’, ‘Metabolic Syndrome X’, ‘Morbid Obesity’, body mass index’, ‘obesity hypoventilation syndrome’, ‘cardiorenal syndrome’, ‘congestive heart failure’, ‘heart failure with preserved ejection fraction’, ‘diastolic dysfunction’ ‘heart ventricle failure’, ‘bariatric surgery’, ‘intentional weight loss’, ‘left ventricle’, ‘left ventricular hypertrophy’, ‘cardiac hypertrophy’, ‘natriuretic peptide’, ‘BNP’ and ‘NT-BNP’. The details are provided in online supplementary 1 The retrieved references were exported to EndNote X7.3, and duplicate citations were removed.
Supplemental material
Inclusion and exclusion criteria
The inclusion criteria were: (1) original articles describing the association of obesity and HF; (2) obesity categories defined according to standard guidelines: underweight, normal BMI, overweight and obese defined as BMI <18.5 kg/m2, 18.5–24.9 kg/m2, 25.0–29.9 kg/m2 and ≥30 kg/m2, respectively. Severe obesity and morbid obesity were defined as BMI >35 kg/m2 and >40 kg/m2, respectively; (3) HF defined as per standard definitions such as ICD-9 or ICD-10, Framingham Heart Study Criteria or European Society of Cardiology (ESC) guideline definition. The exclusion criteria were: (1) acute decompensated HF; (2) studies reporting on RV dysfunction only; (3) BMI categories not defined as per standard guidelines; (4) conference abstracts, editorials, reviews, letters and case reports; (5) small sample size (incidence <5000 patients; prognosis <500 patients and intentional weight loss achieved through bariatric surgery <50 patients); (6) HF prognosis studies of 1 year or less in follow-up duration; (7) intentional weight loss studies that recruited patients with HF in selected population with coronary artery disease or AF only; and (8) intentional weight loss studies with inadequate echocardiographic data. The exclusion of intentional weight loss studies that included patients with AF and coronary artery disease was deemed necessary to provide a representative cohort of obese subjects without cardiac conditions that are impacted by intentional weight loss. Where multiple studies described the same population (substudies and follow-up studies), the study with the most comprehensive data was included.
Study selection and data extraction
The study selection and data extraction were performed by authors (RM and MS), using the predefined inclusion and exclusion criteria. Although review articles were excluded, their reference lists were examined for potential relevant publications. During data extraction, information was collected on the study design, follow-up time, outcome measures, method of assessing outcomes, inclusion/exclusion criteria and results. Where available, the maximally adjusted risk ratios were extracted and pooled across studies. The data were reviewed by two authors independently and disagreements resolved by consensus. The methodological qualities of the included studies were assessed using the Newcastle-Ottawa Scale. The outcomes of the analysis were defined as: (1) incidence of chronic HF across various BMI categories in general population; (2) effect of BMI on cardiovascular (CV) and all-cause mortality in chronic HF in general population; and (3) impact of intentional weight loss achieved via bariatric surgery in obese individuals on cardiac structure and function.
Statistical analysis
Continuous variables are presented as the mean or median and categorical variables as n (%). Separate meta-analyses were performed for: (1) incidence of chronic HF across various BMI categories; (2) effect of BMI on prognosis in chronic HF; and (3) impact of intentional weight loss on adverse cardiac remodelling and indices of myocardial function in obese individuals. Where meta-analysis was not feasible due to small patient or study numbers, raw results were tabulated. A random effects model, using the DerSimonian & Laird method, was used to pool data across studies. Meta-analysis was performed using Review Manager V.5.3. Two meta-analytic effects size types were used for the data analyses, namely: standardised mean difference (SMD) and ORs. SMD was used for reporting association with change in indices of myocardial function as some studies reported indexed values, scaled to body size, rather than absolute values. Back transformation was not always possible. The I2 statistic was used as a measure of variability in observed effect estimates attributable to heterogeneity between the studies.
Results
Search and synthesis of the literature
The online search of PubMed, Embase and Web of Science from 1 January 1950 to 3 April 2018 yielded 4959 citations. Hand searching of references of reviews did not yield additional citations. Of these, 4794 citations were excluded on primary review as they did not meet the inclusion criteria. One hundred and sixty-five citations were identified for secondary review. After removal of studies with sample size less than defined (in exclusion criteria), reviews and non-relevant articles (n=98), BMI categories not defined according to WHO guidelines,8 inadequate data for research questions (n=29) and redundant studies (n=1), 29 studies were included in the final analysis. Of these, 9 studies reported on the association of obesity with HF,2 9–15 11 studies reported on the impact of BMI on prognosis in chronic HF16–26 and 9 studies reported on the impact of intentional weight loss following bariatric surgery on cardiac structure and function.26–34 Figure 1 provides the Consolidated Standards of Reporting Trials flow diagram for the data search.

Search criteria and flow diagram of the literature selection process. BMI, body mass index; HF, heart failure.
Obesity and incidence of HF
Nine studies consisting of 375 056 patients with mean age 53±8 years and follow-up of 12±6 years were analysed.2 9–14 35 36 Two of the studies used ESC guideline criteria for HF diagnosis,13 36 three of the studies used the Framingham Heart Study criteria for diagnosis2 11 12 and the remaining four studies used ICD-9 and ICD-10 criteria for diagnosis.9 10 14 35 Three studies were in diabetic cohorts. Online supplementary 2 provides the study design and the baseline characteristics of patients in studies assessing the incidence of HF in obesity. Insufficient data on left ventricular ejection fraction (LVEF) was reported in these studies. For each categorical BMI group, the incidence of HF was 0.99, 0.34, 0.59, 1.05 and 2.79 cases per 100 person-years for the underweight, normal, overweight, obese and morbid obese groups, respectively. The risk of incident HF (reference group: normal BMI) across BMI categories was 1.22 (95% CI 0.95 to 1.58, p=0.12)), 1.11 (95% CI 0.97 to 1.27, p=0.13), 1.62 (95% CI 1.32 to 1.99, p<0.001) and 1.73 (95% CI 1.30 to 2.31, p<0.001) for underweight, overweight, obese and severely obese individuals, respectively (Figures 2,3A). There was evidence of significant heterogeneity among all comparisons other than that for underweight versus normal BMI.

Increased incidence of HF with obesity. Panels A, B, C and D: HF incidence in underweight, overweight, obese and morbid obese patients with heart failure (HF), respectively.

Panel A: J shaped relationship of obesity and HF incidence. Panel B: U shaped relationship of obesity and cardiovascular mortality in HF with nadir shifted to overweight group.
Impact of obesity on CV and all-cause mortality in HF
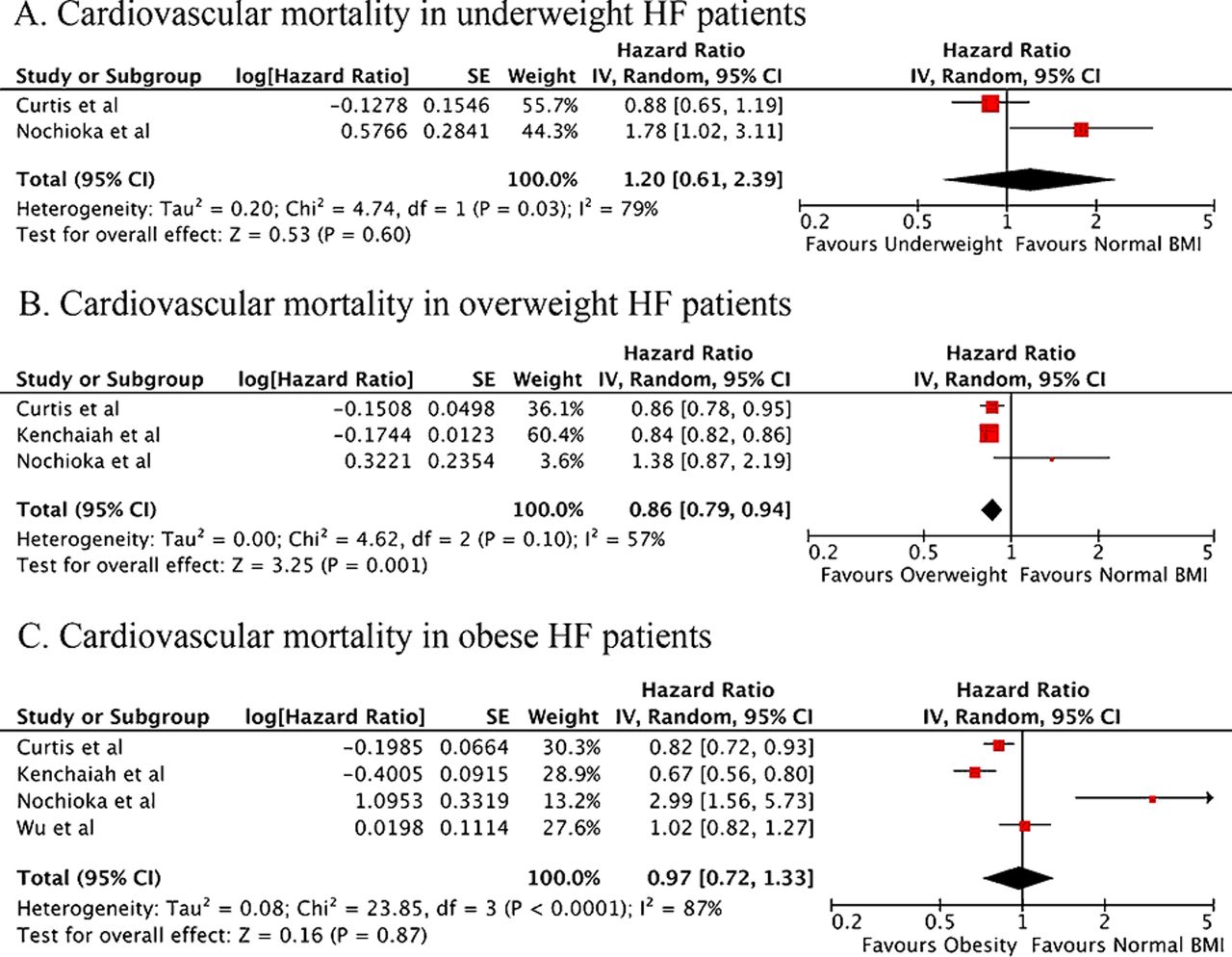
Eleven studies, consisting of 41 019 patients with mean age 67±4 years and follow-up of 4.8±3.4 years, were analysed.16–26 The HRs for CV mortality (reference group: normal BMI) across BMI categories were 1.20 (95% CI 0.61 to 2.39, n=2 studies,16 23 p=0.6), 0.86 (95% CI 0.79 to 0.94); n=3 studies16 21 23 p=0.001) and 0.97 (95% CI 0.72 to 1.33, n=4 studies,16 21 23 26 p=0.87) for underweight, overweight and obese individuals, respectively (Figures 4B,5). The CV mortality was lower in the overweight group relative to normal BMI individuals with absence of significant heterogeneity (I2=57%; p=0.10). However, the CV mortality was not significantly different in the other groups analysed. There was substantial heterogeneity observed in these groups (I2 ≥79%, p≤0.03). Insufficient data were available to perform a meta-analysis on CV mortality in patients considered severely obese.

Obesity and cardiovascular mortality. Panel A, B and C: Cardiovascular mortality in underweight, overweight and obese heart failure patients respectively. BMI, body mass index; CV, cardiovascular; HF, heart failure.

Obesity and all-cause mortality. Panel A, B, C and D: All-cause mortality in underweight, overweight, obese and morbidly-obese heart failure patients respectively.
Table 1 provides the study design and the baseline characteristics of patients in studies assessing the impact of obesity on all-cause mortality in patients with HF. The risk for all-cause mortality was significantly higher in the underweight group with progressive decline in mortality with increase in BMI from underweight to severely obese categories. The HRs for all-cause mortality in HF in underweight, overweight, obese and morbidly obese categories were 1.40 (95% CI 1.25 to 1.57, n=4 studies,16 19 20 p<0.001), 0.88 (95% CI 0.79 to 0.98, n=10 studies,16–25 p=0.02), 0.80 (95% CI 0.69 to 0.91, n=10 studies,16–25 p<0.001) and 0.80 (95% CI 0.77 to 0.83, n=2 studies,20 21 p<0.001), respectively. There was evidence of statistical heterogeneity among included studies in the overweight and obese analyses (p<0.001, I2 >90%). Figure 5 shows the forest plots demonstrating the relationship of all-cause mortality to BMI.
Baseline characteristics of patients in studies assessing the impact of obesity on all-cause mortality in heart failure
Effect of intentional weight loss on cardiac structure and function in obesity
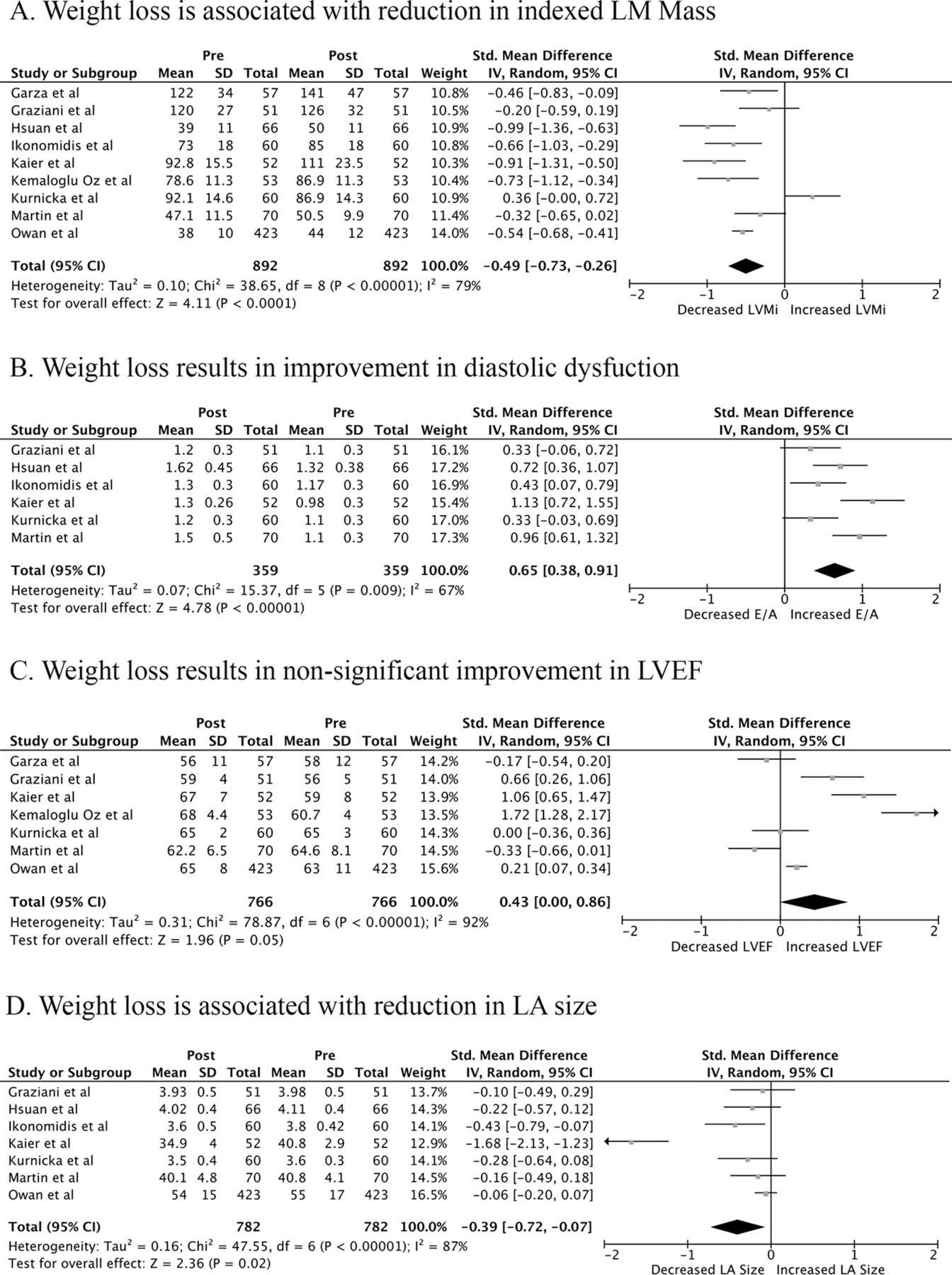
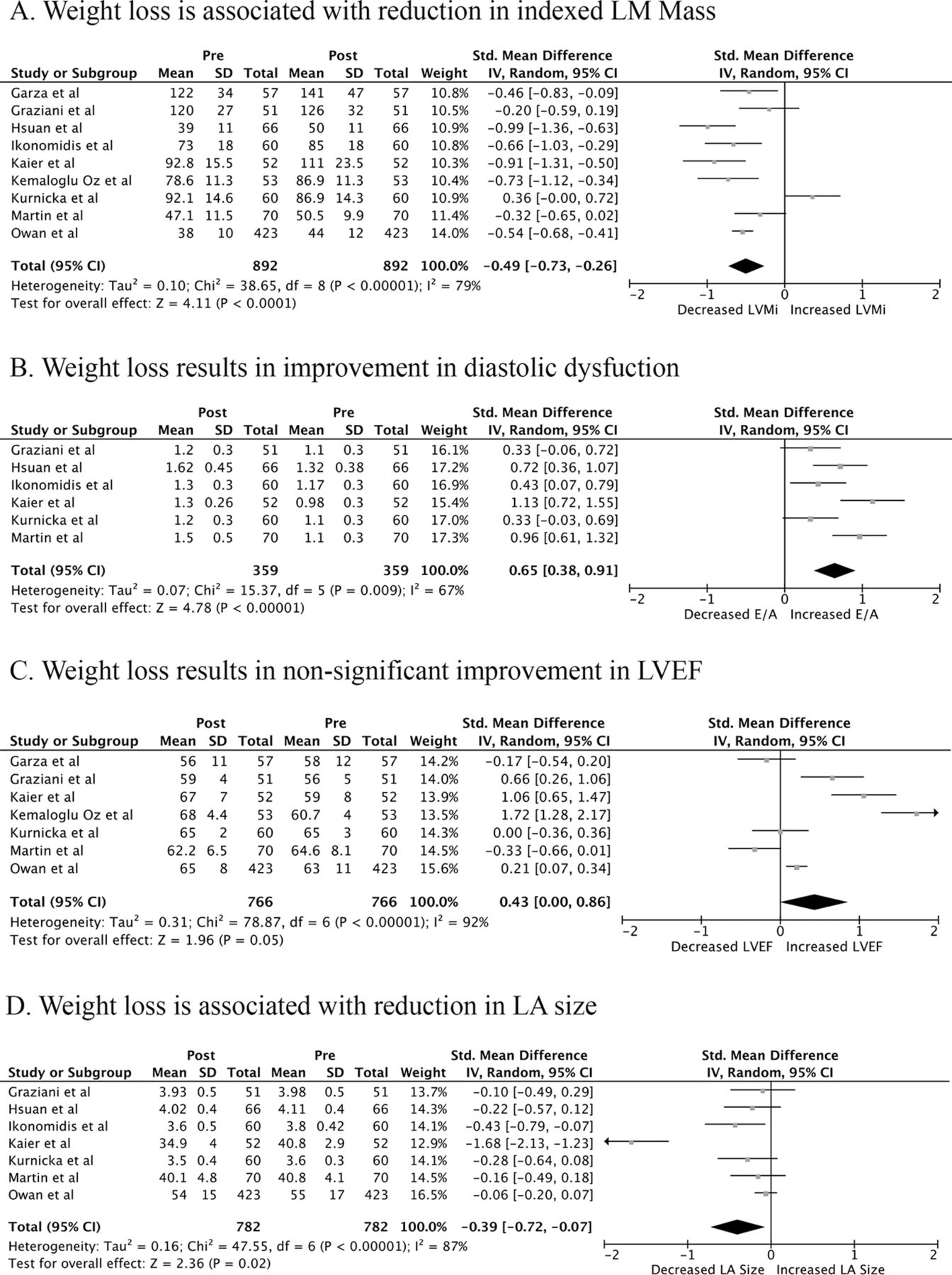
Nine bariatric surgery studies reported intentional weight loss with a mean reduction in weight of 39.4 kg (n=8; 95% CI −45.5 kg to −33.4 kg) and reduction in BMI by 13.6 kg/m2 (n=9; 95% CI −15.6 kg/m2 to −11.6kg/m2) over a mean follow up of 18.1±15.2 months.26–34 The weight loss surgeries used were gastric bypass,26 27 29–31 33 biliopancreatic diversion with duodenal switch,32 gastric sleeve,26 30 33 34 and vertical banded gastroplasty.33 One study did not specify the type of bariatric surgery used.28 Intentional weight loss resulted in reduced left ventricular mass index (SMD −0.49, 95% CI −0.73 to −0.26; p<0.0001), improvement in diastolic function (E/A- SMD 0.65, 95% CI 0.38 to 0.91; p<0.0001) and reduced left atrial size (SMD −0.39, 95% CI −0.72 to −0.07; p=0.02). There was also a non-significant improvement in LVEF (SMD 0.43, 95% CI 0.00 to 0.86; p=0.05). One study compared two different surgical approaches and did not report any difference in outcome. Figure 6 shows the impact of intentional weight loss on cardiac function in obesity.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Intentional weight loss leads to favourable adaptive cardiac remodelling. LVEF, left ventricular ejection fraction.
Study quality and the assessment of risk of bias
All included studies were representative of the relevant cohort with adequate sample size. There was low risk of detection and information biases in all studies. Online supplementary tables 3A, 2B,Cprovides the modified Newcastle Ottawa Score for the included studies.
Discussion
The relationship of obesity with HF is complex with several studies signalling a paradoxical relationship for mortality. The current meta-analysis highlights the increasing risk of HF across the categories of BMI. Despite the higher incidence of HF with obesity, in the presence of established HF, obesity was associated with a paradoxical decline in all-cause mortality. A U-shaped relationship curve was observed between CV mortality and BMI; the overweight cohort experiencing least CV mortality. Importantly, intentional weight loss by bariatric surgery in obese patients resulted in improvement in indices of cardiac structure and myocardial function. The impact of weight loss interventions on clinical outcomes in patients with HF remains unknown.
J-curve relationship between obesity and risk of HF
The current meta-analysis suggests the presence of a ‘J-curve’ relationship between obesity and the risk of incident HF. While there was non-significant 22% and 11% greater risk of incident HF among underweight and overweight participants, respectively, the obese and morbidly obese participants had 62% and 73% greater risk of developing HF.
The mechanisms of HF in obesity are multifactorial. Both experimental and clinical studies have demonstrated that obesity leads to increases in cardiac output and in left heart filling pressures, with subsequent left ventricular hypertrophy and cardiac remodelling resulting in diastolic dysfunction.37 38 Although overt systolic dysfunction is uncommon in the absence of other CV disease, subclinical myocardial dysfunction characterised by decreased systolic mitral annular velocities and reduced longitudinal strain are well described in obesity studies.39 Obesity is also associated with clustering of incident CV risk factors that contribute to the development of ischaemic heart disease, which alone represents a significant aetiological burden of HF. Furthermore, the metabolic syndrome and obstructive sleep apnoea that are frequently present in obese individuals may also contribute to adverse left ventricular loading, dilatation and hypertrophy, pulmonary hypertension and subsequently biventricular failure.37 39 In addition to abnormal loading conditions, epicardial adipose tissue has been shown to infiltrate the underlying cardiac muscle and produce profibrotic and proinflammatory cytokines leading to cardiac remodelling.38 40 These changes develop over several years leading to a steep increase in risk of HF after 10 years of severe obesity.41
Obesity paradox in HF: myth or reality
The obesity paradox has been a long-standing controversy with studies demonstrating lower mortality in obese patients with HF. Horwich et al 3 were the first to report the obesity paradox in HF. Further studies have reported best outcomes in the overweight (BMI 25–29.9) or obese (BMI 30–34.9) categories with increasing mortality seen at the extreme ends of the scale.3 21 23 42 The current meta-analysis confirms the paradoxical decline in all-cause mortality with increasing obesity and demonstrates a U-curve for CV mortality with best outcomes in the overweight group.
The obesity paradox has been attributed to many factors, but the exact mechanisms remain unclear (Box 1). Obese patients may experience greater functional impairment and present early in the course of the disease.16 Similarly, older age, lower use of beta-blocker and ACE inhibitors and cardiac cachexia have been reported in low BMI groups.4 The obesity paradox has been shown to be eliminated, though inconsistently, when adjustments are made for variables such as age, left ventricular function19 and cardiorespiratory reserve.43 Criticism of the obesity paradox in HF includes the observation that much of the data which supports this paradox arises from post hoc analysis of clinical trials designed for different purposes, retrospective studies or the analysis of registries arousing concerns of statistical validity and possible unmeasured confounding induced by selection bias. A lead time bias in diagnosis of HF in the obese and a lower specificity of a HF diagnosis in obese individuals may also impact upon prognostic data. Obese patients with HF possess different clinical and epidemiological profiles compared with normal weight patients with HF, which may impact upon mortality. Thus, comparing HF outcomes on BMI may not account for differences in age, aetiology of HF, LVEF, blood pressure, presence of anaemia, diabetes mellitus, renal function and nutritional status where differences are present when comparing obese versus non-obese individuals.44
Intentional weight loss in obese HF cohort
The observation of the obesity paradox in HF has raised scepticism on any potential therapeutic benefit from intentional weight loss in obese patients with HF. However, a recent large Swedish registry has provided robust data on the beneficial effects of intentional weight loss in the prevention of HF development in obese patients.5 This study demonstrated a graded decrease in the risk of incident HF with weight loss. A weight loss of 10 kg was associated with a 23% lower risk of developing HF. In concurrence with this study, the current meta-analysis showed that intentional weight loss in obesity resulted in improvement in diastolic function and reduction in LV mass as well as left atrial size. This reverse and favourable cardiac remodelling may potentially avert the future development of HF in obesity. The weight loss was achieved with bariatric surgery in the studies included in the meta-analysis.
Notably, there is a striking lack of significant clinical studies on the direct role of intentional weight loss in established HF. However, the potential benefit of intentional weight loss as a therapeutic intervention in HF is suggested by a few bariatric surgical studies in patients with HF. First, Vest et al reported retrospective data from 42 patients with left ventricular systolic dysfunction (LVEF <50%) who underwent bariatric surgery with a mean follow-up period of 23 months. Bariatric surgery resulted in a reduction in BMI of 11 kg/m2 and a mean LVEF improvement of 5.1% with no significant cardiac adverse events.45 Similarly, improvement in LVEF has been demonstrated in other small case series in obese patients with HF.46 47 In addition, reduction in HF hospitalisation by intentional weight loss by bariatric surgery has been demonstrated in a recently published self-controlled series of 524 patients with HF and a range of LVEFs.48 Intentional weight loss achieved via non-surgical approaches (via caloric restriction and/or aerobic exercise training) has also been found to be beneficial in improving peak oxygen uptake, in patients with HF-PEF.49 Similarly, a small study of a 6-month dietary-led interventional weight loss programme in 34 obese chronic HF patients whereby a modest weight loss of 3 kg was achieved resulted in improvements in functional assessments as well as LVEF.50 Further substantial clinical data are required to determine whether weight loss achieved via differing surgical or non-surgical approaches results in differing haemodynamic effects and clinical outcomes in the HF population.
Clinical implications
Intentional weight loss has been previously shown to be beneficial in obese patients with other CV disorders such as AF.7 8 The current meta-analysis shows that obesity is associated with HF, and intentional weight loss leads to favourable cardiac remodelling in the obese. It also demonstrates the least CV mortality in HF in the overweight group. Hence, this meta-analysis provides theoretical data with regard to potential prognostic benefit from intentional weight loss in obese patients with HF. This information may be crucial in designing studies to evaluate the role of intentional weight loss in such a cohort.
Limitations
Although BMI is the most common anthropometric measure of adiposity, it does not accurately distinguish between body fat and lean mass, and the relation between BMI and body fat varies with age, gender and ethnicity. Furthermore, undernutrition may be present in patients classified as obese on the basis of BMI. Despite the limitations, the BMI was the most suitable measure to conduct this meta-analysis. Several studies did not report the aetiology of HF, which is a crucial factor determining prognosis. In addition, the studies did not provide differentiation between HF with reduced ejection fraction and HF preserved ejection fraction. Furthermore, there were insufficient studies to conduct an analysis for CV mortality in morbidly obese patients with HF. There are also too few studies to draw definite conclusions regarding weight management in HF. Although the bariatric surgery studies provided evidence for improvement in a number of cardiac indices, there was a paucity of information on improvement in outcomes in HF. Finally, the assessment of left atrial size from the measurement of a left atrial diameter from the parasternal long-axis imaging was used in the bariatric surgery studies. This measurement, while regularly performed in routine echocardiography, is prone to angulation and foreshortening. It has been essentially superseded by an indexed volumetric assessment (left atrial volume, indexed to body surface area), in echocardiographic laboratories.
Conclusion
Obesity is associated with an increased risk of developing HF. Despite the elevated risk, a paradoxical decline in all-cause mortality is observed. Similarly, a U-shaped curve exists for CV mortality with best outcome evident in the overweight group. Intentional weight reduction results in improvement in indices of cardiac structure and function in obese individuals free of HF. Given the burgeoning population incidence of HF, adequately powered and appropriately designed studies to assess the effects of intentional weight loss in obese patients with HF are urgently required.
Obesity paradox and heart failure
Support of the obesity paradox in heart failure
High volume clinical registry data indicating a lower mortality in overweight and mildly obese individuals with heart failure.
Cardiac cachexia a poor prognostic feature in heart failure.
Potential protective effects of: tumour necrosis factor-alpha (secreted from adipose tissue).
Increased tolerability of disease modifying and prognostic pharmacotherapies in the obese.
Controversial aspects and possible explanations obesity paradox in heart failure
Lower specificity of heart failure diagnosis in the obese.
Lead time bias in diagnosis of heart failure in the obese.
Different clinical and epidemiological profile of heart failure in the obese.
Statistical validity of large study data, predominantly with body mass index.
Inherent limitations of body mass index alone as a measure of obesity.
Key messages
What is already known on this subject?
The management of obesity in heart failure is controversial.
What might this study add?
The meta-analysis confirms the increased risk of HF with obesity and presence of an ‘obesity paradox’ for all-cause mortality. Intentional weight loss improves indices of cardiac function.
How might this impact on clinical practice?
Collider stratification bias, lead time bias and different baseline characteristics may explain the obesity paradox. There are no data to suggest detrimental effect of intentional weight loss in obese patients with heart failure. Further studies are required to evaluate the role of intentional weight loss in obese patients with heart failure.
References
Footnotes
DL and PS contributed equally.
RM and MS contributed equally.
Contributors RM, MS, AE, DL and PS had full access to all the data in the study and take responsibility for the integrity of the data and accuracy of the data analysis. Study concept and design: RM and PS. Acquisition of data: RM and MS. Analysis and interpretation of data: RM, MS, AE, DL and PS. Drafting of manuscript: RM, MS and PS. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: RM, MS and AE. Study supervision: RM and PS.
Funding This study was supported by funds from the Centre of Heart Rhythm Disorders at the University of Adelaide. RM is supported by an Early Career Fellowship from the National Health and Medical Research Council (NHMRC) and National Heart Foundation (NHF) of Australia and by the Leo J. Mahar Lectureship by the University of Adelaide. MS is supported by the Dawes Scholarship from the Royal Adelaide Hospital. AE and JH are supported by the Early Career Fellowship from NHF of Australia. DAM is supported by the Robert J. Craig Scholarship from the University of Adelaide and by the Indonesia Endowment Fund for Education, Ministry of Finance, The Republic of Indonesia. KBK is supported by Asia Pacific Heart Rhythm Society and the New Zealand Heart Foundation overseas fellowship. JH is supported by the Derek Frewin Lectureship from the University of Adelaide. DL is supported by a Beacon Research Fellowship from the University of Adelaide. CG is supported a Fellowship from the University of Adelaide. DK is supported by a Senior Research Fellowship from the NHMRC. DL is supported by the Robert J. Craig Lectureship from the University of Adelaide. PS is supported by Practitioner Fellowships from the NHMRC and by the NHF of Australia. The sponsor of the study is the University of Adelaide. Several of the authors are employees of the University of Adelaide. The sponsor has had no direct involvement in the management or outcomes of the study.
Competing interests The University of Adelaide reports receiving on behalf of RM lecture and/or consulting fees from Abbott and Medtronic. The University of Adelaide reports receiving on behalf of RM research funding from Abbott and Medtronic. DL reports having served on the advisory board of LivaNova and Medtronic. The University of Adelaide reports receiving on behalf of DL reports lecture and/or consulting fees from LivaNova, Medtronic, Pfizer and ResMed. The University of Adelaide reports receiving on behalf of DL research funding from Sanofi, ResMed and Medtronic. PS reports having served on the advisory board of Biosense-Webster, Medtronic, Abbott, Boston Scientific and CathRx. The University of Adelaide reports receiving on behalf of PS lecture and/or consulting fees from Biosense-Webster, Medtronic, Abbott and Boston Scientific. The University of Adelaide reports receiving on behalf of PS research funding from Medtronic, Abbott, Boston Scientific, Biotronik and Liva Nova.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no data in this work.
Patient consent for publication Not required.